


CIO #117
Ozempic and body composition in elderly, obese, diabetic subjects; Cardio and muscle-loss; and More

Check Out What I’ve Been Checking Out
The Best of What I’m Reading
“The Effectiveness of GLP-1 Receptor Agonist Semaglutide on Body Composition in Elderly Obese Diabetic Patients: A Pilot Study”
If you’ve regularly consumed mainstream and/or social media in the past year, you’ve likely heard about GLP-1 agonists—like semaglutide—the class of Type 2 Diabetes medications that have become widely used for weight-loss.
Though GLP-1 agonists do appear to facilitate weight-loss, likely via their appetite suppression, I have heard and read about concerns that a significant amount of the weight lost is coming from decreases in muscle mass.
Since—as you’ve seen me continuously emphasize—muscle mass and strength are important for both lifespan and healthspan, this would be a significant drawback for GLP-1 agonists.
Out of curiosity, I’ve begun to look through some GLP-1 research, like the study above, to form an opinion for myself on whether this is a legitimate concern.
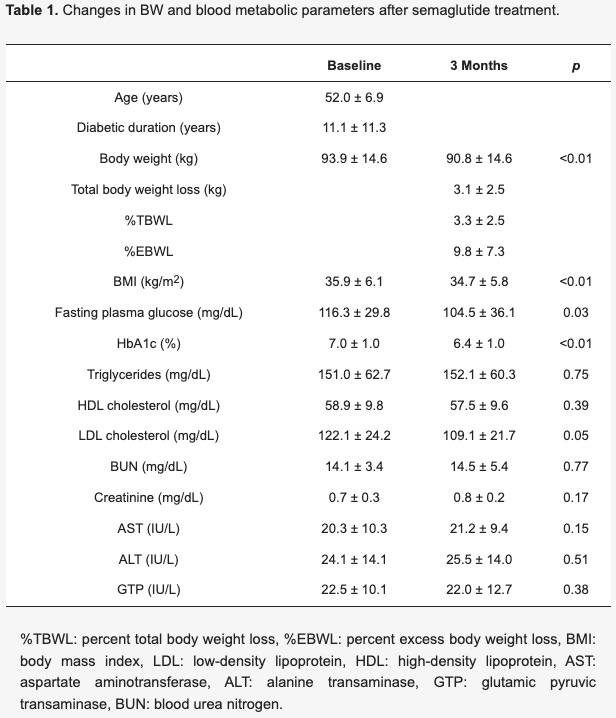
In this case, Ozeki and Colleagues followed 13 obese subjects with Type 2 diabetes (average age: ~52) for 3-months of semaglutide use. (I)
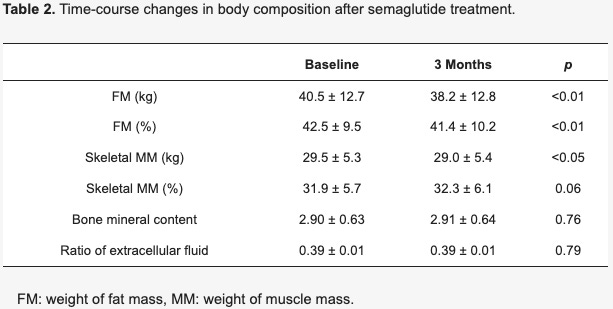
On average, these subjects lost ~6.8 lbs, of which ~5 lbs was fat mass and ~1.0 lb was skeletal muscle mass, according to bio electric impedance measurements (this is the same technology behind the handlebar devices you may have used before to measure your body fat percentage). (I)
Interestingly, the subjects also statistically significantly improved their fasting blood glucose levels, low-density lipoprotein cholesterol levels, and HbA1c (a longer term marker of blood glucose levels). (I)
So, it seems there were significant benefits in terms of metabolic markers and fat loss (though, some might argue that 5 lbs in 3 months isn’t extremely impressive), but are they worth the muscle mass lost?
To be fair, the authors do cite that reducing calories normally without using GLP-1 agonists leads to muscle mass losses as well:
“In contrast to fat loss, a reduction in skeletal muscle is not good for diabetic obese patients. In general, losses in FM and MM occur after caloric restriction and bariatric surgery” (I)
And, they mention that, though the muscle mass losses seem low in their particular study, some other studies found greater muscle mass losses from GLP-1 agonist use:
“studies of the effects of GLP1-RAs on LBM and MM have produced relatively inconsistent findings. In the LEAD-3 trial, liraglutide decreased body weight after treatment and induced loss of LBM [24]. There are also studies reporting no change, or increases, in LBM after liraglutide treatment [27,28]. Similar to liraglutide, the relative contribution of fat weight to body weight loss induced by exenatide ranged from 40% [33] to 52% [34]. Other studies reported a small increase in LBM after exenatide treatment in patients with T2DM [35]. The loss of fat weight was greater than the TBW decrease and was accompanied by an increase in skeletal muscle [36]. Our study also demonstrated that %MM is conserved in subjects treated with semaglutide.” (I)
I plan on diving in deeper to get some more data before developing a firm opinion, so stay tuned for more on the topic.
The Best of What I’m Watching
“How To Do Cardio (Without Losing Muscle)”
(click the title to watch)
“Why vitamin D trials are flawed and how to fix them”
(click the title to watch)
How much stronger does caffeine make you?
Recent Video Content From Shortcut U
How does weight-loss relate to water weight and muscle mass?
(click the title to watch)
Talking Studies #004: Blood Pressure Measurement Details

Last time in the Talking Studies Series, we talked through the Sprint Blood Pressure Trial, which suggests that more intensive blood pressure lowering to less than 120 mm Hg systolic reduces risk of cardiovascular disease and death as compared to standard blood pressure lowering to 140 mm Hg systolic.